Third spacing refers to the pathological shift of intravascular fluid into the interstitial and extracellular compartments, leading to hypovolemia despite total body fluid excess. During cardiopulmonary bypass (CPB), this phenomenon is exacerbated by inflammatory responses, hemodilution, and capillary leak syndrome, significantly affecting perfusion management and postoperative recovery.
Pathophysiology of Third Spacing in CPB
Pathophysiology of Third Spacing in Cardiopulmonary Bypass (CPB)
Third spacing refers to the pathological shift of intravascular fluid into the interstitial and extracellular compartments. This phenomenon is particularly pronounced during cardiopulmonary bypass (CPB) due to the systemic inflammatory response, capillary leak, hemodilution, and altered fluid dynamics. Understanding the pathophysiological mechanisms behind third spacing is crucial for optimizing fluid management strategies during cardiac surgery.
1. Systemic Inflammatory Response Syndrome (SIRS) and Capillary Leak
CPB triggers a systemic inflammatory response syndrome (SIRS) due to multiple factors, including:
- Exposure of blood to non-endothelial surfaces (oxygenator, tubing, reservoirs)
- Mechanical trauma from the roller or centrifugal pump
- Ischemia-reperfusion injury during aortic cross-clamping and subsequent myocardial reperfusion
- Hemodilution from the priming solution
- Hypothermia and subsequent rewarming, affecting vascular permeability
These events activate the inflammatory cascade, leading to:
✔ Cytokine release: Interleukin-6 (IL-6), Tumor Necrosis Factor-alpha (TNF-α), Interleukin-1β (IL-1β) → Increased vascular permeability
✔ Complement activation: C3a, C5a → Stimulates neutrophils and mast cells → Capillary damage
✔ Endothelial dysfunction: Nitric oxide (NO) and reactive oxygen species (ROS) disrupt endothelial tight junctions
✔ Histamine release: Increases vasodilation and fluid extravasation
This capillary leak syndrome results in massive plasma fluid extravasation, leading to hypovolemia despite total body fluid overload.
2. Hemodilution and Oncotic Pressure Imbalance
During CPB, hemodilution occurs due to:
✔ Large priming volumes (~1000–1500 mL in adults, even more in pediatrics) diluting blood components
✔ Crystalloid-based prime solutions lowering plasma oncotic pressure
✔ Loss of albumin due to CPB circuit interactions
Plasma oncotic pressure, primarily maintained by albumin, is crucial for keeping fluid inside the vasculature. However, hemodilution reduces oncotic pressure, resulting in:
🚨 Shift of intravascular fluid into interstitial spaces
🚨 Pulmonary and peripheral edema
🚨 Reduced preload and cardiac output post-CPB
In neonates and infants undergoing congenital heart surgery, this effect is even more pronounced due to their inherently higher capillary permeability and lower plasma protein reserves.
3. Hypothermia, Vasodilation, and Rewarming Effects
Hypothermia (used during CPB for organ protection) causes:
- Peripheral vasoconstriction → Temporary preservation of intravascular volume
- Reduced metabolism → Lower oxygen demand
However, rewarming post-CPB leads to:
🔥 Sudden vasodilation → Capillary leak exacerbation
🔥 Increased permeability → Fluid shifts into interstitial compartments
🔥 Tissue edema (lungs, gut, kidneys, brain) → Organ dysfunction
This effect explains why many patients develop hypotension and require vasopressor support after CPB termination.
4. The Role of the Lymphatic System
Normally, the lymphatic system counteracts third spacing by returning interstitial fluid to circulation. However, during CPB:
🚨 Lymphatic clearance is overwhelmed due to massive fluid extravasation
🚨 Pulmonary lymphatics fail to clear excess lung water → Leading to pulmonary edema
🚨 Delayed postoperative diuresis → Prolonged ICU stays and fluid overload
5. Organ-Specific Consequences of Third Spacing in CPB
| Organ System | Effects of Third Spacing |
|---|---|
| Lungs | Pulmonary edema, impaired gas exchange, difficult ventilatory weaning |
| Heart | Reduced preload, low cardiac output syndrome (LCOS), hypotension |
| Kidneys | Acute kidney injury (AKI) due to hypoperfusion, reduced urine output |
| Gastrointestinal | Bowel edema, delayed gastric emptying, impaired nutrient absorption |
| Brain | Cerebral edema, altered mental status, increased risk of stroke |
The pathophysiology of third spacing during CPB involves a complex interplay of inflammation, capillary leak, hemodilution, hypothermia-induced vasoconstriction, and rewarming vasodilation. Understanding these mechanisms allows for targeted interventions such as ultrafiltration, oncotic pressure modulation, and controlled fluid resuscitation, ultimately improving patient outcomes post-cardiac surgery.
Risk Factors Contributing to Third Spacing
Risk Factors Contributing to Third Spacing in Cardiopulmonary Bypass (CPB)
Third spacing during cardiopulmonary bypass (CPB) is influenced by multiple factors that exacerbate fluid shifts from the intravascular space into the interstitial and extracellular compartments. Understanding these risk factors helps perfusionists and cardiac surgical teams develop proactive strategies to mitigate postoperative complications like hypovolemia, tissue edema, and hemodynamic instability.
1. Prolonged Cardiopulmonary Bypass Time
⏳ The longer the patient remains on CPB, the greater the inflammatory response and fluid shift.
- Extended CPB (>2–3 hours) increases exposure to the circuit → More mechanical trauma and blood contact with non-endothelial surfaces → Triggers systemic inflammatory response syndrome (SIRS)
- Prolonged ischemia-reperfusion injury → Exaggerates endothelial dysfunction and capillary leak
- Leads to excessive cytokine release (IL-6, TNF-α, IL-1β, C-reactive protein) → Increased vascular permeability
💡 Clinical Implication: Patients with long CPB durations often require higher doses of vasopressors, aggressive ultrafiltration, and careful fluid balance management to stabilize hemodynamics postoperatively.
2. High Prime Volume & Hemodilution
💧 Large prime volumes dilute plasma proteins, leading to reduced oncotic pressure and excessive interstitial fluid accumulation.
- Adult CPB prime volume: 1000–1500 mL
- Pediatric/neonatal CPB prime volume: Higher relative to circulating blood volume → Greater hemodilution impact
- Use of crystalloid-based primes further reduces albumin concentration, promoting fluid leakage into tissues
- Decreased hematocrit (Hct) and hemoglobin (Hb) levels → Impaired oxygen delivery and hemodynamic instability
💡 Clinical Implication:
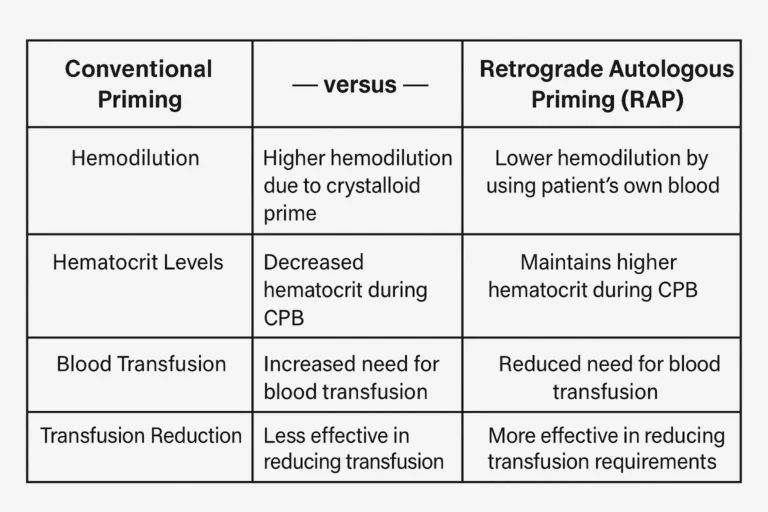
- Minimizing prime volume (retrograde autologous priming – RAP) and using colloids like albumin helps maintain intravascular volume.
- Hemoconcentration via ultrafiltration (MUF, CUF) is essential in pediatric cases to prevent fluid overload.
3. Low Oncotic Pressure & Hypoalbuminemia
⚠️ Low oncotic pressure promotes fluid movement out of the vasculature into the interstitial space, worsening third spacing.
- Serum albumin <3.0 g/dL before surgery → Increased capillary leak
- Excessive crystalloid resuscitation intraoperatively → Further dilution of oncotic proteins
- Low oncotic pressure exacerbates pulmonary and peripheral edema, leading to difficult ventilatory weaning and prolonged ICU stays
💡 Clinical Implication:
- Preoperative albumin supplementation in at-risk patients can mitigate fluid shifts.
- Colloid-based priming solutions (albumin, hydroxyethyl starch) may help maintain oncotic pressure.
4. Hypothermia and Rewarming Effects
🌡️ Temperature management during CPB significantly influences vascular permeability and fluid shifts.
- Hypothermia (28–32°C) is used to reduce metabolic demand during bypass → Leads to peripheral vasoconstriction → Temporary intravascular volume preservation
- During rewarming (>36°C), sudden vasodilation occurs, leading to:
✔ Increased capillary leak
✔ Reduced systemic vascular resistance (SVR) → Hypotension
✔ Worsened third spacing
💡 Clinical Implication:
- Gradual and controlled rewarming is essential to prevent excessive vasodilation.
- Vasopressors (norepinephrine, vasopressin) may be needed post-bypass to counteract hypotension from fluid shifts.
5. Pre-Existing Conditions & Patient-Specific Factors
Certain comorbidities and patient characteristics significantly increase third spacing risk:
🫀 Congestive Heart Failure (CHF)
- Elevated venous pressures and pre-existing fluid overload make patients more susceptible to excessive interstitial edema post-CPB.
- Diuretic therapy before surgery can help optimize fluid balance.
🩸 Chronic Kidney Disease (CKD)
- Impaired renal function prevents effective fluid clearance, leading to persistent third spacing postoperatively.
- Dialysis-dependent patients may require intraoperative hemofiltration.
🦠 Sepsis & Systemic Inflammatory Conditions
- Septic patients already have heightened capillary permeability and low oncotic pressure.
- CPB-induced inflammation further worsens vascular leakage.
👶 Pediatric Patients (Neonates & Infants)
- Higher capillary permeability & immature endothelial barrier → Increased fluid shifts
- Smaller blood volume relative to prime volume → More significant hemodilution
- Greater susceptibility to SIRS → Worsened inflammatory response
💡 Clinical Implication:
- Tailoring fluid strategies for high-risk patients is essential to reduce postoperative complications.
6. Pediatric Population: Increased Capillary Permeability
👶 Infants and neonates undergoing congenital heart surgery experience more severe third spacing due to:
- Immature endothelial tight junctions → More prone to fluid leakage
- Higher metabolic rate and increased inflammatory response
- Large prime volume relative to blood volume, leading to severe hemodilution
💡 Clinical Implication:
- Aggressive ultrafiltration (Modified Ultrafiltration – MUF) is critical in pediatric cases to remove excess fluid and inflammatory mediators.
7. Excessive Crystalloid Use Postoperatively
🚨 Overzealous crystalloid administration post-CPB worsens third spacing and fluid overload.
- Crystalloids (Ringer’s lactate, normal saline) lack oncotic properties, driving fluid shifts into tissues.
- Leads to pulmonary edema, prolonged ventilation, and delayed ICU discharge.
- Balanced fluid resuscitation strategies (albumin-guided resuscitation, early diuresis) are essential to prevent volume overload.
💡 Clinical Implication:
- Monitor lactate clearance, urine output, and hemodynamic parameters to guide postoperative fluid therapy.
- Early diuresis with loop diuretics (furosemide, bumetanide) prevents prolonged third spacing effects.
📌 Third spacing during CPB is driven by multiple factors, including prolonged bypass time, hemodilution, inflammation, hypothermia, and patient-specific conditions.
📌 Understanding these risk factors allows for targeted strategies such as oncotic pressure optimization, ultrafiltration, and controlled fluid resuscitation to improve patient outcomes.
📌 Tailored management, especially in high-risk groups like pediatric and renal-compromised patients, is crucial for reducing postoperative complications.
Several factors increase susceptibility to third spacing during CPB:
- Prolonged bypass time → Higher inflammatory activation
- High prime volume → Greater hemodilution
- Low oncotic pressure → Reduced intravascular fluid retention
- Hypothermia → Vasoconstriction followed by vasodilation post-rewarming
- Pre-existing conditions (CHF, CKD, sepsis, malnutrition)
- Pediatric patients → Increased capillary permeability and fluid shifts
Clinical Implications and Hemodynamic Consequences
Clinical Implications and Hemodynamic Consequences of Third Spacing in Cardiopulmonary Bypass (CPB)
Third spacing during cardiopulmonary bypass (CPB) leads to significant fluid shifts from the intravascular compartment into the interstitial and extracellular spaces. This process results in hypovolemia, hemodynamic instability, and tissue edema, affecting both intraoperative management and postoperative recovery.
Understanding the clinical implications and hemodynamic consequences of third spacing is crucial for perfusionists, anesthesiologists, and cardiac surgeons to implement effective management strategies.
1. Hemodynamic Instability Post-CPB
🔴 Hypovolemia & Hypotension
- Despite total body fluid overload, the patient often presents intravascularly depleted due to third spacing.
- Reduced preload → Leads to low cardiac output syndrome (LCOS) and hypotension upon weaning from CPB.
- Reflex tachycardia may occur as a compensatory mechanism but is often ineffective due to decreased stroke volume.
- Hypovolemia-induced systemic vasodilation can further exacerbate hemodynamic collapse, requiring vasopressor and inotropic support.
💡 Management Approach:
✅ Careful volume replacement with colloids (albumin) or blood products if hematocrit is low.
✅ Use of vasopressors (norepinephrine, vasopressin) to maintain systemic vascular resistance (SVR).
✅ Hemoconcentration via ultrafiltration to restore intravascular volume.
2. Pulmonary Edema & Respiratory Dysfunction
🫁 Third spacing leads to excessive interstitial lung water accumulation, causing pulmonary congestion and impaired gas exchange.
Pathophysiology:
- CPB-induced capillary leak increases alveolar fluid accumulation.
- Hemodilution and low oncotic pressure worsen pulmonary edema.
- Increased lung stiffness (decreased compliance) → Higher ventilatory pressures required postoperatively.
- Hypoxemia and prolonged ventilatory support increase the risk of postoperative pulmonary complications.
💡 Clinical Signs:
✔ Dyspnea, low oxygen saturation (SpO₂), frothy pulmonary secretions
✔ Difficult ventilator weaning
✔ Chest X-ray showing bilateral pulmonary infiltrates
💡 Management Approach:
✅ Restrictive fluid administration postoperatively to prevent worsening pulmonary edema.
✅ Early use of diuretics (furosemide, bumetanide) to promote fluid mobilization.
✅ Use of positive end-expiratory pressure (PEEP) and lung-protective ventilation strategies.
3. Peripheral & Tissue Edema
💧 Third spacing contributes to widespread tissue edema, affecting multiple organ systems.
- Peripheral edema (hands, legs, face) due to fluid accumulation in soft tissues.
- Gut edema → Reduced intestinal perfusion → Risk of ileus, delayed gastric emptying, and malabsorption.
- Cerebral edema (in severe cases) → May lead to increased intracranial pressure (ICP), confusion, and delayed neurological recovery.
💡 Management Approach:
✅ Early mobilization and elevation of extremities to reduce peripheral edema.
✅ Controlled fluid resuscitation to avoid unnecessary overload.
✅ Albumin-guided fluid therapy to maintain oncotic pressure.
4. Delayed Recovery & Increased ICU Length of Stay
📉 Prolonged third spacing effects lead to a longer ICU stay due to:
- Prolonged mechanical ventilation due to respiratory compromise.
- Higher risk of postoperative infections from excessive fluid shifts and immune suppression.
- Need for prolonged inotropic support due to persistent hypotension and capillary leak syndrome.
- Delayed return of kidney function in patients with fluid overload.
💡 Management Approach:
✅ Proactive fluid balance monitoring with daily weight and fluid intake-output tracking.
✅ Early diuresis to prevent excessive interstitial fluid accumulation.
✅ Close monitoring of hemodynamic parameters (MAP, CVP, lactate clearance) to optimize perfusion.
5. Increased Risk of Multi-Organ Dysfunction Syndrome (MODS)
🚨 Severe third spacing contributes to impaired organ perfusion, increasing the risk of multi-organ failure.
- Acute Kidney Injury (AKI):
- Low renal perfusion pressure due to hypovolemia → Prerenal AKI.
- Fluid overload-induced interstitial edema worsens renal function.
- Liver Dysfunction:
- Hepatic congestion from fluid shifts leads to cholestasis and increased liver enzymes.
- Poor splanchnic perfusion causes gut ischemia and bacterial translocation.
- Neurological Dysfunction:
- Cerebral edema leads to confusion, delayed awakening, and cognitive dysfunction.
- Increased blood-brain barrier permeability exacerbates postoperative delirium.
💡 Management Approach:
✅ Optimize hemodynamics with goal-directed fluid therapy.
✅ Maintain MAP >65 mmHg to ensure adequate organ perfusion.
✅ Use of vasopressors as needed to maintain end-organ perfusion.
📌 Third spacing during CPB has profound hemodynamic and clinical consequences, including hypovolemia, pulmonary edema, tissue swelling, and increased ICU stays.
📌 Understanding these effects allows for targeted interventions such as ultrafiltration, controlled fluid therapy, and optimized hemodynamic support.
📌 A proactive approach to managing third spacing can significantly improve postoperative outcomes and reduce complications.
Unchecked third spacing leads to:
- Hypovolemia & hypotension post-CPB
- Tissue edema (lungs, gut, brain)
- Difficult ventilatory weaning due to pulmonary congestion
- Increased ICU stay & fluid overload syndromes
Strategies for Managing Third Spacing During Cardiopulmonary Bypass (CPB)
Third spacing during cardiopulmonary bypass (CPB) leads to fluid shifts from the intravascular compartment into the interstitial and extracellular spaces, causing hypovolemia, tissue edema, and hemodynamic instability. Effective management strategies aim to minimize fluid loss, maintain oncotic pressure, and optimize hemodynamic stability to improve patient outcomes.
A multimodal approach is essential, including preoperative, intraoperative, and postoperative interventions, along with mechanical and pharmacological methods to regulate fluid balance.
1. Preoperative Optimization
🔹 The goal of preoperative management is to minimize the patient’s risk of excessive third spacing by optimizing volume status and reducing inflammatory responses before surgery.
✅ Albumin Supplementation
- Indication: Patients with low oncotic pressure (hypoalbuminemia) are at a higher risk of fluid extravasation during CPB.
- Action: Administering IV albumin (5% or 25%) preoperatively helps maintain intravascular volume and reduces interstitial fluid accumulation.
✅ Diuretic Therapy in CHF & Fluid-Overloaded Patients
- Patients with congestive heart failure (CHF) or fluid retention (renal dysfunction, liver disease) benefit from preoperative loop diuretics (furosemide, bumetanide) to reduce excess total body fluid.
- Action: Helps prevent excessive hemodilution and postoperative pulmonary congestion.
✅ Steroid Administration to Reduce Inflammation
- CPB triggers a systemic inflammatory response syndrome (SIRS), worsening third spacing.
- Action: Preoperative corticosteroids (e.g., methylprednisolone 30 mg/kg IV) reduce inflammation, capillary leak, and fluid shifts.
2. Intraoperative Management
🔹 The focus during CPB is to minimize hemodilution, maintain oncotic pressure, and reduce inflammatory responses.
✅ Minimized Prime Volume in CPB Circuit
- Large priming volumes dilute plasma proteins, lowering oncotic pressure and promoting third spacing.
- Action: Use low-prime circuits and albumin-augmented priming solutions to reduce hemodilution.
- Alternative: Hemoconcentration during CPB can maintain hematocrit levels.
✅ Colloid Administration (Albumin or Hydroxyethyl Starch) Instead of Excessive Crystalloids
- Crystalloids (Ringer’s lactate, saline) distribute rapidly into the interstitial compartment, exacerbating third spacing.
- Action: Albumin or hydroxyethyl starch (HES) can be used to maintain intravascular volume.
- Caution: HES should be used selectively due to potential nephrotoxicity in high doses.
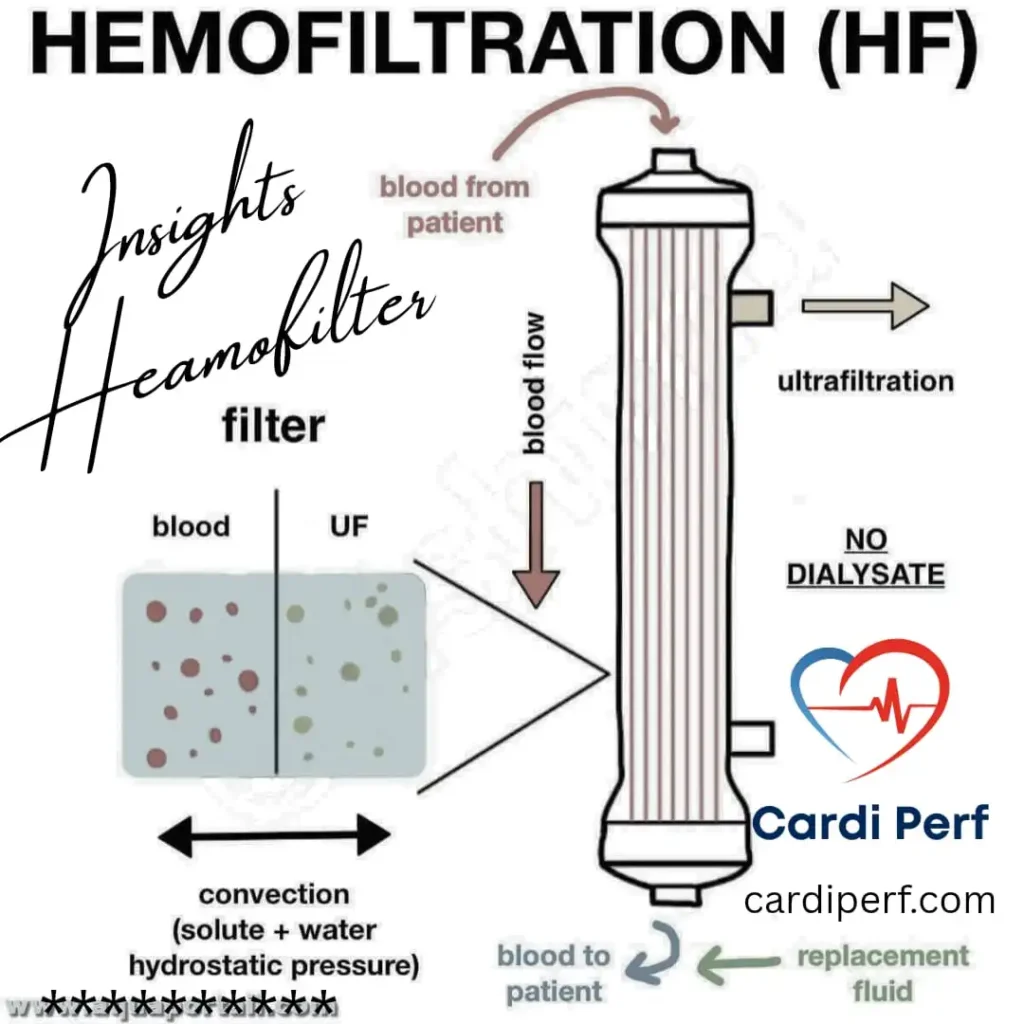
✅ Ultrafiltration & Hemoconcentration During CPB
- Ultrafiltration removes excess plasma water while concentrating proteins and blood components, reducing edema and improving hemodynamic stability.
- Types of Ultrafiltration Used:
🔹 Conventional Ultrafiltration (CUF) → Removes excess water during CPB.
🔹 Modified Ultrafiltration (MUF) → Used post-CPB, particularly beneficial in pediatric patients to remove inflammatory mediators and reduce lung water content.
✅ Temperature Management to Prevent Excessive Vasodilation
- Hypothermia during CPB leads to vasoconstriction, and rapid rewarming causes vasodilation, exacerbating third spacing.
- Action: Controlled rewarming (≤0.5°C per 5 minutes) prevents excessive capillary leak and hypotension.
✅ Vasopressor Support to Maintain Perfusion Pressure
- Excessive vasodilation post-CPB worsens intravascular volume loss.
- Action: Use vasopressors like norepinephrine or vasopressin to maintain systemic vascular resistance (SVR) and prevent hypotension.
3. Postoperative Strategies
🔹 The goal postoperatively is to mobilize third-spaced fluid back into circulation, enhance diuresis, and prevent excessive interstitial edema.
✅ Controlled Fluid Resuscitation (Avoiding Aggressive Crystalloids)
- Excessive fluid administration worsens interstitial edema and delays ventilator weaning.
- Action: Use colloid-based resuscitation (albumin) instead of excessive crystalloid infusion.
✅ Early Diuresis to Mobilize Third-Spaced Fluid
- Loop diuretics (furosemide, bumetanide) are used to enhance urine output and reduce tissue edema.
- Action: Helps with pulmonary decongestion and peripheral edema resolution.
- Caution: Monitor for electrolyte imbalances (hypokalemia, hypomagnesemia).
✅ Monitoring Perfusion Markers (Lactate Clearance, CVP, Urine Output)
- Key indicators of fluid balance include:
✔ Lactate clearance → Measures perfusion adequacy.
✔ Central venous pressure (CVP) → Helps guide fluid therapy.
✔ Urine output → Indicator of effective diuresis and renal function.
✅ Targeted Albumin Administration to Restore Intravascular Volume
- Administering albumin postoperatively helps pull third-spaced fluid back into circulation, improving hemodynamic stability and oxygen delivery.
4. Role of Pharmacological Agents in Managing Third Spacing
Pharmacological therapy plays a key role in reducing inflammatory response, promoting diuresis, and maintaining intravascular volume.
| Drug Category | Examples | Mechanism of Action |
|---|---|---|
| Colloids | Albumin (5%, 25%) | Maintains oncotic pressure, pulls fluid back into circulation |
| Diuretics | Furosemide, Bumetanide | Promotes diuresis, reduces interstitial edema |
| Steroids | Methylprednisolone | Reduces inflammation, decreases capillary leak |
| Vasopressors | Norepinephrine, Vasopressin | Maintains systemic vascular resistance (SVR), prevents hypotension |
| Anti-inflammatory Agents | Pentoxifylline, NSAIDs | Reduce cytokine release, decrease vascular permeability |
Summary: Key Takeaways
✅ Preoperative: Optimize volume status with albumin, diuretics, and steroids to reduce inflammatory response.
✅ Intraoperative: Minimize hemodilution, use ultrafiltration, and regulate vasopressor therapy for hemodynamic stability.
✅ Postoperative: Focus on controlled fluid resuscitation, early diuresis, and monitoring perfusion markers.
✅ Pharmacological Support: Use albumin, diuretics, steroids, and vasopressors as needed.
By implementing these strategies, perfusionists, anesthesiologists, and cardiac surgical teams can effectively manage third spacing, reducing postoperative complications and improving patient recovery. 🚀
Preoperative Optimization
- Albumin supplementation (if hypoalbuminemia is present) to maintain oncotic pressure
- Diuretics in CHF patients to reduce preoperative congestion
- Steroids & anti-inflammatory agents to blunt SIRS response
Intraoperative Management
- Minimized priming volume → Reducing hemodilution
- Maintaining oncotic pressure → Use of colloids like albumin or hydroxyethyl starch
- Hemoconcentration via ultrafiltration → Balances fluid shifts
- Careful temperature management → Avoid excessive vasodilation post-rewarming
- Vasopressor support (if required) → Maintain adequate perfusion pressures
Postoperative Strategies
- Controlled fluid resuscitation → Avoid aggressive crystalloid use
- Early diuresis & hemoconcentration → Prevent pulmonary congestion
- Monitoring of lactate clearance & perfusion indices → Guide fluid therapy
- Targeted albumin administration → To restore intravascular volume
Role of Ultrafiltration and Hemoconcentration
Modified Ultrafiltration (MUF) & Conventional Ultrafiltration (CUF) are essential techniques in reducing third spacing effects:
- Increases hematocrit → Improves oxygen delivery
- Removes inflammatory mediators → Reduces capillary leak
- Reduces pulmonary edema → Enhances postoperative recovery
In pediatric cardiac surgery, MUF is particularly beneficial in reducing post-CPB edema and improving hemodynamic stability.
Pharmacological Approaches to Third Spacing
- Albumin Infusion → Maintains oncotic pressure, reducing fluid extravasation
- Furosemide/Bumetanide (Loop Diuretics) → Promotes diuresis, counteracting interstitial overload
- Steroids (Methylprednisolone) → Reduces SIRS and capillary permeability
- Vasopressors (Norepinephrine, Vasopressin) → Counteracts post-CPB vasodilation
FAQs with answers on Managing Third Spacing in CPB: Fluid Control Strategies:
1. What is third spacing, and why is it a concern during CPB?
Answer: Third spacing refers to the pathological shift of fluid from the intravascular space into the interstitial and extracellular compartments, leading to relative hypovolemia despite total body fluid excess. During cardiopulmonary bypass (CPB), factors like hemodilution, systemic inflammatory response syndrome (SIRS), and capillary leak syndrome exacerbate third spacing, causing hypotension, tissue edema, and organ dysfunction.
2. What are the primary causes of third spacing in CPB?
Answer: The key contributors to third spacing during CPB include:
- Systemic Inflammatory Response Syndrome (SIRS): Blood exposure to the bypass circuit triggers inflammation.
- Capillary Leak Syndrome: Increased capillary permeability leads to fluid extravasation.
- Hemodilution: Large prime volumes dilute intravascular oncotic pressure.
- Hypothermia & Rewarming: Affects vascular permeability and fluid dynamics.
- Low Oncotic Pressure: Reduces the ability to retain intravascular fluid.
3. How does third spacing impact hemodynamics during and after CPB?
Answer: Third spacing causes:
- Hypovolemia & Hypotension: Fluid shifts reduce circulating volume, leading to low perfusion pressure.
- Tissue Edema: Pulmonary, cerebral, and gut edema impair oxygenation and organ function.
- Difficult Ventilation: Pulmonary congestion increases post-op ventilation time.
- Increased ICU Stay: Fluid overload extends recovery and may lead to complications like ARDS or renal dysfunction.
4. What role does ultrafiltration play in managing third spacing?
Answer: Ultrafiltration (UF) is crucial in fluid removal and inflammation control during CPB:
- Conventional Ultrafiltration (CUF): Removes excess water while CPB is running.
- Modified Ultrafiltration (MUF): Used after CPB to remove inflammatory mediators and excess fluid, improving hemodynamics.
- Hemoconcentration: Increases hematocrit and oncotic pressure, reducing third spacing effects.
5. How can perfusionists minimize third spacing during CPB?
Answer: Perfusionists can adopt these strategies:
- Use minimal prime volume to reduce hemodilution.
- Incorporate colloids (e.g., albumin) in prime to maintain oncotic pressure.
- Optimize ultrafiltration to remove excess fluids and inflammatory mediators.
- Monitor and adjust perfusion pressures to maintain adequate capillary flow.
- Control temperature fluctuations to reduce vascular permeability changes.
6. What preoperative strategies can reduce third spacing in CPB?
Answer: Pre-op management includes:
- Albumin supplementation if hypoalbuminemia is present.
- Diuretics in CHF patients to prevent preoperative congestion.
- Steroids or anti-inflammatory agents to blunt the inflammatory response.
- Nutritional optimization to improve protein levels and vascular integrity.
7. How does temperature management impact third spacing?
Answer:
- Hypothermia (during CPB): Causes vasoconstriction, reducing capillary leakage.
- Rewarming (post-CPB): Leads to vasodilation, worsening third spacing.
- Controlled rewarming prevents excessive vasodilation and fluid shifts.
8. What pharmacological interventions help manage third spacing?
Answer:
- Albumin infusion: Maintains intravascular oncotic pressure.
- Diuretics (furosemide, bumetanide): Helps with fluid mobilization postoperatively.
- Steroids (methylprednisolone): Reduces inflammation and capillary leak.
- Vasopressors (norepinephrine, vasopressin): Maintains perfusion pressure post-CPB.
9. How can postoperative management prevent complications from third spacing?
Answer:
- Controlled fluid resuscitation: Avoid excessive crystalloid administration.
- Early diuresis & hemoconcentration: Prevents pulmonary congestion.
- Monitoring perfusion indices: Guides fluid therapy and vasopressor use.
- Targeted albumin administration: Helps restore intravascular volume.
10. What are the key takeaways for managing third spacing in CPB?
Answer:
✅ Pre-op: Optimize oncotic pressure & reduce inflammation risk.
✅ Intra-op: Use minimal prime, ultrafiltration, and temperature control.
✅ Post-op: Manage fluid shifts carefully with diuretics, vasopressors, and albumin.
✅ Team Approach: Perfusionists, anesthesiologists, and surgeons must coordinate for optimal outcomes.
Conclusion
Effective management of third spacing during CPB requires a multimodal approach, including fluid balance optimization, ultrafiltration, and pharmacological intervention. By proactively addressing fluid shifts, perfusionists and cardiac surgical teams can enhance hemodynamic stability, reduce postoperative complications, and optimize patient recovery.
Call to Action:
🚀 Stay ahead in perfusion science! Subscribe to cardiperf.com for in-depth insights into cutting-edge perfusion strategies! 🔥