Retrograde Autologous Priming (RAP) has emerged as a pivotal technique in blood conservation during cardiopulmonary bypass (CPB). This method involves displacing the priming solution in the bypass circuit with the patient’s own blood before initiating bypass, thereby reducing hemodilution and blood transfusion requirements.
As part of patient blood management (PBM), RAP has been explored for its potential to decrease reliance on homologous blood transfusion, which is often linked to increased morbidity and mortality in cardiac surgery.
Table of Contents
How RAP Works in Cardiopulmonary Bypass (CPB)
Bypass Circuit Priming: The Role of Priming Solution in CPB
Traditionally, the CPB circuit is primed with a crystalloid or colloid solution to ensure adequate circulation upon initiation. However, this can lead to hemodilution, reducing hematocrit levels and requiring blood transfusions.
The priming solution typically consists of balanced salt solutions, colloids (such as albumin or hydroxyethyl starch), or a combination of both. While necessary for initiating bypass, this additional volume dilutes the patient’s circulating blood, leading to lower hemoglobin levels and an increased likelihood of requiring red blood cell transfusions. Hemodilution can also result in reduced plasma oncotic pressure, causing fluid shifts that contribute to post-operative edema and impaired oxygen delivery to tissues.
To mitigate these effects, perfusionists seek strategies like RAP, which allows partial or complete replacement of the priming solution with the patient’s own blood, thereby reducing unnecessary dilution and preserving essential clotting factors.
The Mechanism of RAP
RAP works by using the patient’s own circulating blood to replace the crystalloid prime:
- Venous cannula displacement (Antegrade RAP): Blood from the venous system displaces priming solution into a reservoir.
- Arterial cannula displacement (Retrograde RAP): Blood is slowly infused backward from the aortic cannula, displacing the priming solution from the arterial side.

The process is conducted carefully to avoid hemodynamic instability. As the priming solution is withdrawn, it is essential to monitor the patient’s arterial pressure, central venous pressure (CVP), and oxygenation to ensure that RAP does not induce hypotension or compromise organ perfusion. A slow and controlled withdrawal of crystalloid, combined with volume shifts from the patient’s own intravascular stores, ensures that perfusion remains stable.
How to perform RAP technique
Retrograde Autologous Priming (RAP) is a technique used in cardiac surgery to reduce hemodilution and the need for homologous blood transfusions during cardiopulmonary bypass (CPB).
Key Aspects of RAP:
- Purpose:
- Minimizes priming volume of the CPB circuit by displacing crystalloid prime with the patient’s own blood.
- Reduces hemodilution and preserves hematocrit, lowering the risk of transfusion.
- Procedure:
- Before initiating CPB, blood is drained retrograde (backward) from the arterial line into the venous reservoir.
- This displaces the crystalloid prime, replacing it with the patient’s autologous blood.
- Advantages:
- Decreased hemodilution and better hematocrit levels.
- Lower risk of transfusion-related complications.
- Reduced inflammatory response due to less foreign priming fluid.
- Disadvantages & Challenges:
- Requires careful monitoring to avoid air entrapment.
- May not be suitable for all patients (e.g., those with severe anemia or hypovolemia).
- Can be technically demanding.
- Clinical Applications:
- Commonly used in adult and pediatric cardiac surgery.
- Particularly beneficial in patients at high risk for transfusion or with low body weight.
Conclusion:
RAP is an effective blood conservation strategy in CPB, improving outcomes by reducing hemodilution and transfusion needs. Proper execution is essential to avoid complications.
Would you like more details on any specific aspect?
Steps for Performing Retrograde Autologous Priming (RAP) in Cardiopulmonary Bypass (CPB)
Retrograde Autologous Priming (RAP) is a blood conservation technique used to reduce hemodilution during cardiac surgery. Below are the key steps:
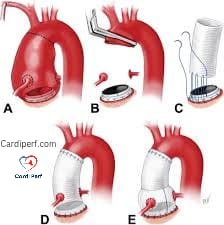
1. Preparation Before CPB Initiation
- Ensure the CPB circuit is primed with crystalloid solution (e.g., balanced electrolyte solution).
- Connect arterial and venous lines to the patient (aortic cannula and venous cannula, respectively).
- Verify that all air is purged from the circuit.
2. Displacement of Crystalloid Prime (Retrograde Filling)
- Step 1: Clamp the venous line (prevents blood from draining into the reservoir prematurely).
- Step 2: Slowly initiate arterial blood flow from the patient backward (retrograde) into the CPB circuit by:
- Allowing arterial blood to flow retrograde through the arterial line into the venous reservoir.
- Alternatively, using a syringe or roller pump to withdraw blood gently.
- Step 3: As autologous blood fills the circuit, the crystalloid prime is displaced and drained from the venous reservoir.
- Target: Typically, 300–500 mL of crystalloid is replaced with the patient’s blood (varies based on circuit size and patient blood volume).
3. Completion of RAP and Transition to Full CPB
- Step 4: Once sufficient autologous blood has replaced the crystalloid, clamp the arterial line.
- Step 5: Unclamp the venous line and begin standard venous drainage.
- Step 6: Initiate full CPB as usual.
4. Monitoring & Safety Checks
- Avoid Air Embolism: Ensure no air is entrained during retrograde filling.
- Hemodynamic Stability: Monitor blood pressure, as RAP may transiently reduce preload.
- Hematocrit Check: Confirm improved hemodilution parameters post-RAP.
Advantages of RAP
✔ Reduces hemodilution & transfusion needs
✔ Preserves coagulation factors
✔ Lowers inflammatory response
Potential Risks
✖ Hypotension during blood withdrawal
✖ Risk of air embolism if not performed carefully
✖ Not suitable for anemic or hemodynamically unstable patients
Conclusion
RAP is an effective method to minimize hemodilution in CPB. Proper execution requires careful blood displacement while maintaining patient stability.
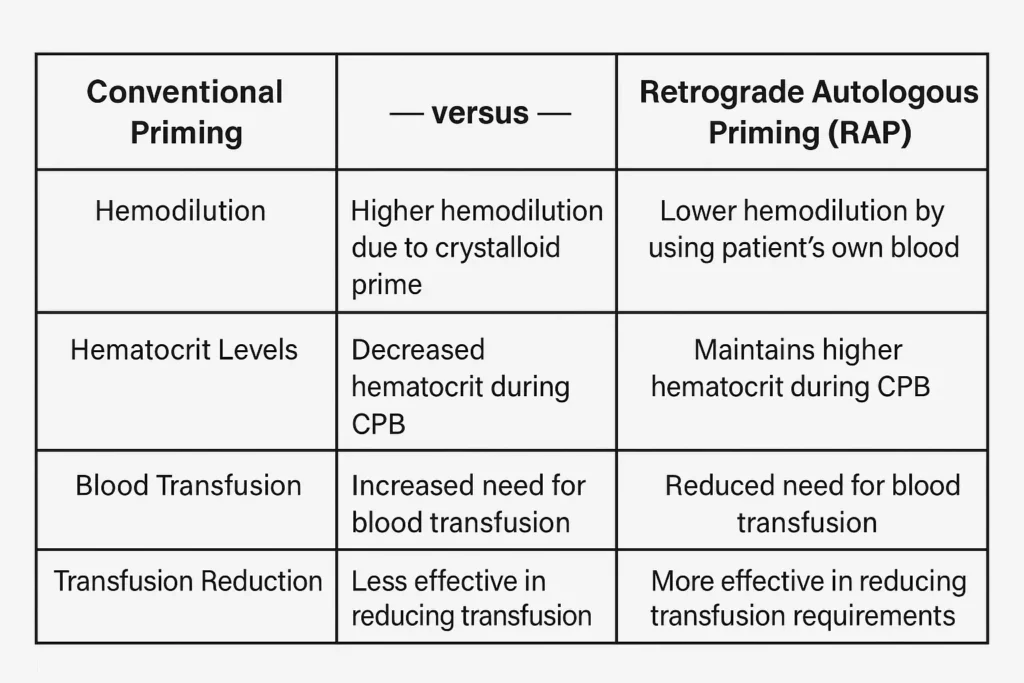
Comparison with Conventional Priming Methods
| Feature | Conventional Priming | Retrograde Autologous Priming (RAP) |
|---|---|---|
| Priming Volume | High (Crystalloid-based) | Reduced (Blood displacement) |
| Hemodilution | Significant | Minimized |
| Transfusion Need | Higher | Lower |
| Hematocrit Impact | Decreased | Maintained |
The Impact of RAP on Hemodilution & Hematocrit
- How RAP reduces priming volume and affects hematocrit levels
- The connection between hemodilution and transfusion requirements
- Advantages of higher hematocrit during CPB
Does RAP Reduce Homologous Blood Transfusion?
One of the primary benefits of retrograde autologous priming is the reduction of hemodilution, leading to higher hematocrit levels during bypass. Studies indicate that replacing 800-1000 mL of priming solution with autologous blood can significantly improve intraoperative hematocrit, reducing the need for transfusions.
Why Higher Hematocrit Matters?
- Improved oxygen delivery to tissues
- Reduced risk of coagulopathy and excessive bleeding
- Lower incidence of postoperative complications
When hematocrit is maintained at optimal levels during CPB, it supports better microcirculatory perfusion and oxygenation of critical organs, reducing the risk of complications such as acute kidney injury (AKI) and prolonged mechanical ventilation. By avoiding extreme hemodilution, RAP helps sustain systemic vascular resistance (SVR) and ensures stable perfusion pressure, crucial for patients with pre-existing comorbidities such as anemia or chronic renal insufficiency.
Additionally, maintaining a higher hematocrit reduces inflammatory responses triggered by excessive fluid dilution. Since blood transfusions can introduce inflammatory mediators and immunogenic substances, minimizing transfusion requirements through RAP contributes to better postoperative recovery and reduced hospital stays.
Does RAP Reduce Homologous Blood Transfusion?
Multiple systematic reviews and meta-analyses suggest that RAP reduces blood transfusion requirements in cardiac surgery patients by limiting the dilutional effect of crystalloid priming.
Clinical Evidence Supporting RAP
- Randomized controlled studies show a 30–50% reduction in transfusion rates among patients undergoing RAP.
- Observational studies indicate a lower incidence of inflammatory responses linked to transfusion.
- Morbidity and mortality rates appear unchanged, supporting RAP as a safe alternative to conventional priming.
Safety & Efficacy of RAP in Cardiac Surgery
Is RAP Safe? Understanding the Risks
While RAP has shown promising results, there are concerns regarding:
- Hypotension risk during priming displacement
- Variable success rates based on patient hemodynamics
- Exclusion criteria: Patients with low cardiac output syndrome or severe vascular disease
Current Guidelines & Best Practices in Perfusion Techniques
Leading cardiac surgery guidelines recommend RAP as a viable method for reducing transfusion dependence. However, perfusionists must tailor its use based on patient-specific factors such as baseline hematocrit, volume status, and hemodynamic stability.
Future of Retrograde Autologous Priming in Perfusion Science
The future of retrograde autologous priming is promising, with ongoing research and clinical trials evaluating its expanded applications in minimally invasive cardiac surgery (MICS) and hybrid perfusion techniques.
Innovations on the Horizon
- Smart perfusion monitoring systems integrating real-time hematocrit analysis
- Automated RAP protocols to enhance consistency
- Combination with other blood conservation strategies, such as miniaturized CPB circuits
Conclusion: Is RAP the Future of Blood Conservation in CPB?
Retrograde Autologous Priming (RAP) is a game-changing technique that reduces hemodilution, maintains hematocrit, and minimizes transfusion needs during cardiopulmonary bypass. While further research is required, current data strongly support its safety and efficacy, making RAP an essential component of patient blood management strategies in modern cardiac surgery.
Key Takeaways:
✅ RAP significantly reduces priming volume and limits hemodilution.
✅ Studies show up to 50% reduction in transfusion needs.
✅ Safety considerations include hemodynamic stability and patient selection.
✅ RAP is increasingly recognized as a best practice in perfusion science.
📢 Are you using RAP in your CPB protocols? Share your experiences in the comments below!
Frequently Asked Questions (FAQs) on Retrograde Autologous Priming (RAP)
- What is Retrograde Autologous Priming (RAP)?
RAP is a blood conservation technique in cardiopulmonary bypass (CPB) where the priming solution in the bypass circuit is displaced with the patient’s own blood before initiating bypass. This reduces hemodilution and the need for blood transfusion. - How does RAP help in reducing blood transfusions?
By replacing crystalloid prime with the patient’s own blood, RAP maintains a higher hematocrit level during CPB, reducing the dilutional effect and lowering the need for homologous blood transfusions. - Does RAP increase hematocrit during surgery?
Yes, RAP helps maintain a higher hematocrit level by preventing excessive dilution of red blood cells, ensuring better oxygen delivery and reducing postoperative complications. - Is RAP safe for all patients undergoing cardiac surgery?
While RAP is generally safe, it may not be suitable for patients with low cardiac output, severe vascular disease, or hemodynamic instability, as withdrawing priming volume may cause hypotension. - What is the difference between Retrograde and Antegrade Autologous Priming?
- Retrograde Autologous Priming (RAP): Blood is infused backward from the arterial cannula, pushing the priming fluid out of the circuit.
- Antegrade Autologous Priming (AAP): Blood displaces the priming solution from the venous cannula forward into the circuit.
- What are the risks associated with RAP?
The primary risks include transient hypotension during the priming process and potential difficulty in complete priming displacement in certain patients with low blood volume. - Does RAP affect postoperative recovery?
Yes, studies suggest that RAP reduces the need for blood transfusion, which in turn decreases the risk of transfusion-related inflammatory responses, leading to better recovery and shorter hospital stays. - What are the best practices for performing RAP safely?
- Monitor arterial pressure and central venous pressure (CVP) during displacement.
- Withdraw the priming solution gradually to prevent hypotension.
- Use RAP selectively based on patient hemodynamics and blood volume status.
- Is RAP widely used in all cardiac surgery centers?
While RAP is gaining recognition and is recommended in blood conservation strategies, its adoption varies depending on institutional protocols, surgeon preferences, and perfusion team experience. - Can RAP be used in pediatric cardiac surgeries?
Yes, but with caution. Pediatric patients have a smaller blood volume, so careful monitoring is required to avoid excessive volume shifts and maintain stable perfusion.
Conclusion: Is RAP the Future of Blood Conservation in CPB?
Retrograde Autologous Priming (RAP) is proving to be an essential technique in modern perfusion science, offering a reliable method to reduce hemodilution, maintain hematocrit, and minimize the need for blood transfusions. By integrating RAP into patient blood management strategies, hospitals can lower transfusion-related risks, improve postoperative recovery, and promote better patient outcomes.
While RAP implementation depends on institutional protocols and perfusionist expertise, its growing body of evidence supports its routine use in CPB. As advances in perfusion technology continue, automated RAP systems, real-time hematocrit monitoring, and hybrid blood conservation strategies will likely enhance its effectiveness, making RAP a cornerstone of cardiac surgery blood management in the future.