Cardiovascular diseases remain one of the leading causes of death worldwide, with coronary artery disease (CAD) being a major contributor. When patients present with significant coronary artery blockages, two primary treatment options are available: Coronary Artery Bypass Grafting (CABG) and Percutaneous Coronary Intervention (PCI). As a perfusionist or cardiac health professional, understanding the nuances of these treatments, their indications, and outcomes is crucial for optimal patient care.
In this article, we’ll dive deep into the differences between CABG and PCI, explore their advantages, and provide insight into which patients are suitable candidates for each procedure.
What is Coronary Artery Bypass Grafting (CABG)?
Coronary Artery Bypass Grafting (CABG) is a type of surgery used to treat patients with severe coronary artery disease (CAD). During the procedure, a surgeon creates a new path for blood to flow around a blocked or narrowed coronary artery. The bypass is created using a healthy blood vessel taken from another part of the patient’s body, such as the leg (saphenous vein), chest (internal mammary artery), or forearm (radial artery).
Key Indications for CABG:
- Multiple vessel disease or left main coronary artery disease.
- Patients with severe blockage that cannot be treated effectively with PCI.
- Cases where long-term outcomes, such as survival, are better with surgery.
- Patients with diabetes who often benefit more from CABG than PCI.
Benefits of CABG:
- Provides long-term relief and may improve survival in patients with severe coronary disease.
- Better outcomes in patients with multi-vessel disease.
- Less need for repeated interventions compared to PCI.
What is Percutaneous Coronary Intervention (PCI)?
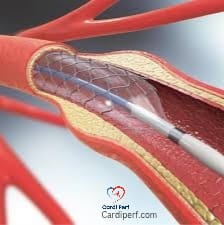
Percutaneous Coronary Intervention (PCI), commonly known as angioplasty, is a non-surgical procedure that involves threading a catheter through the blood vessels to the coronary arteries to open up blocked or narrowed arteries. A balloon is inflated to widen the artery, and in many cases, a stent is placed to keep the artery open.
Key Indications for PCI:
- Single or two-vessel coronary artery disease without severe blockage.
- Patients with less complex coronary lesions.
- Acute coronary syndrome (e.g., STEMI or NSTEMI) where quick intervention is required.
- Patients who are poor surgical candidates or have high surgical risk.
Benefits of PCI:
- Less invasive than CABG, with quicker recovery times.
- Shorter hospital stays.
- Suitable for patients with lower risk and less extensive disease.
CABG vs. PCI: Key Differences
While both CABG and PCI aim to improve blood flow to the heart, there are key differences between the two procedures. Let’s break them down:
- Invasiveness:
- CABG: A major surgical procedure that involves opening the chest and requires a longer recovery period.
- PCI: A minimally invasive procedure that only requires small incisions and usually involves less recovery time.
- Effectiveness for Multi-Vessel Disease:
- CABG: More effective in patients with multi-vessel disease or left main coronary artery disease, as it can bypass several blockages at once.
- PCI: Works best for patients with single or two-vessel disease but may not be as effective in more complex cases.
- Long-Term Results:
- CABG: CABG generally provides better long-term outcomes in terms of survival and freedom from further revascularization, especially in patients with complex coronary anatomy.
- PCI: While PCI provides immediate relief, it may require follow-up procedures, particularly if stents become occluded or restenosis occurs.
- Recovery Time:
- CABG: Typically requires a hospital stay of 5-7 days, with several weeks of recovery time.
- PCI: Recovery is faster, often requiring only a one-day hospital stay, with most patients resuming normal activities within a week.
Choosing Between CABG and PCI: Patient Selection
The decision between CABG and PCI depends on multiple factors, including the patient’s overall health, the severity and location of the coronary blockages, and the patient’s risk factors. Here’s a breakdown of when each treatment might be preferred:
- CABG is preferred in patients with:
- Severe multi-vessel coronary artery disease.
- Left main coronary artery disease.
- Diabetes (especially if the patient has complex coronary anatomy).
- A history of prior PCI failure.
- PCI is preferred in patients with:
- Single or two-vessel disease with low complexity.
- Acute coronary syndrome (e.g., STEMI) requiring urgent intervention.
- High surgical risk or contraindications to surgery.
Emerging Trends and Technologies in CABG and PCI
Advancements in technology are continuously improving the outcomes of both CABG and PCI. For CABG, robotic-assisted surgery, off-pump CABG, and minimally invasive techniques are reducing recovery times and improving precision. On the PCI side, drug-eluting stents and bioresorbable stents are improving long-term outcomes by reducing the risk of restenosis.

FAQs about Coronary Artery Bypass Grafting (CABG) vs. PCI
1. What is the difference between CABG and PCI?
Answer:
CABG (Coronary Artery Bypass Grafting) is a surgical procedure where a bypass is created to reroute blood around blocked coronary arteries using healthy blood vessels from another part of the body. PCI (Percutaneous Coronary Intervention) is a minimally invasive procedure that uses a catheter to open blocked arteries, typically with a balloon or stent.
2. Which procedure is better for treating coronary artery disease (CAD)?
Answer:
Both CABG and PCI are effective treatments for CAD, but the choice depends on the severity and complexity of the coronary blockages. CABG is generally preferred for multi-vessel disease or left main coronary artery disease, while PCI is suitable for single or two-vessel disease with less complex blockages.
3. How long does recovery take after CABG?
Answer:
Recovery after CABG typically takes 6–8 weeks. Patients may need to stay in the hospital for 5–7 days, followed by several weeks of recovery at home. Full recovery, including returning to normal activities, can take up to three months.
4. How long does recovery take after PCI?
Answer:
Recovery after PCI is much quicker than CABG. Most patients are able to leave the hospital within 24–48 hours and can resume normal activities within 1–2 weeks, depending on individual circumstances.
5. What are the risks associated with CABG?
Answer:
CABG carries the risks typical of any major surgery, including infection, bleeding, blood clots, stroke, heart attack, and complications from anesthesia. Long-term risks include graft failure or a need for additional procedures.
6. What are the risks associated with PCI?
Answer:
PCI is less invasive but still carries risks such as bleeding at the catheter insertion site, allergic reactions to contrast dye, vessel damage, stent thrombosis, or restenosis (re-narrowing of the artery). In rare cases, patients may experience a heart attack or stroke during the procedure.
7. What are the benefits of CABG over PCI?
Answer:
CABG is generally more effective in patients with multi-vessel coronary disease, left main coronary artery disease, or those with diabetes. It tends to provide longer-lasting results with a lower likelihood of needing future interventions compared to PCI.
8. Can PCI be used to treat all patients with coronary artery disease?
Answer:
No, PCI is most effective for patients with single or two-vessel disease and less complex blockages. It may not be suitable for patients with severe multi-vessel disease or left main coronary artery disease, where CABG may be the better option.
9. Can a patient have both CABG and PCI?
Answer:
Yes, in some cases, a patient may require both procedures. For example, PCI may be performed to treat specific blockages, and CABG may be used for more extensive coronary artery disease, especially when PCI is not suitable for certain areas.
10. Are there alternatives to CABG and PCI for treating coronary artery disease?
Answer:
Yes, lifestyle changes (such as diet, exercise, and smoking cessation), medications (like statins and blood thinners), and emerging treatments like enhanced external counterpulsation (EECP) may be used. However, for severe cases of CAD, CABG or PCI remains the most effective intervention.
Conclusion
In the battle of CABG vs. PCI, there is no one-size-fits-all answer. Both procedures offer significant benefits, but their effectiveness depends on the patient’s individual circumstances. As a cardiac professional, your role in determining the most appropriate treatment is crucial for ensuring the best possible outcomes for patients with coronary artery disease.
For perfusionists and other cardiac healthcare professionals, staying informed about these procedures and the latest advancements in technology is essential for providing top-tier care. Whether you’re working in the operating room with CABG patients or assisting in the cath lab during PCI, your expertise is vital in optimizing treatment and improving patient survival and quality of life. For update keep visiting cardiperf.com