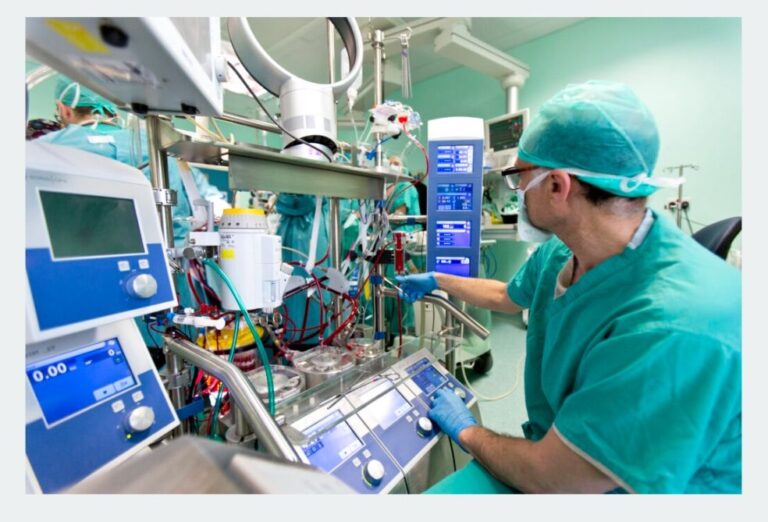
Blood Gas Analyzer
Recommendations
Reference Ranges
- pH: 7.35 – 7.45
- pCO₂: 35 – 45 mmHg
- pO₂ (On Pump): 250 – 300 mmHg
- Base Excess: -2 to +2 mmol/L
- Potassium (K⁺): 3.5 – 4.5 mmol/L (Pediatric), 4.5 – 5.5 mmol/L (Adult)
- Hemoglobin: 12 – 16 g/dL (Female), 13.5 – 17.5 g/dL (Male)
- Hemoglobin on Pump: 7.5 – 9.5 g/dL
Arterial blood gas (ABG) analysis is a critical tool in the operating room, providing real-time insights into a patient’s oxygenation, ventilation, and acid-base status during cardiac procedures. For perfusionists, mastering ABG interpretation is essential to optimize cardiopulmonary bypass (CPB) management, ensure patient safety, and improve surgical outcomes. This detailed guide dives deep into ABG interpretation for perfusionists, offering actionable insights, clinical correlations, and best practices tailored to the cardiac surgery environment.
Understanding the Importance of ABG Interpretation for Perfusionists
In cardiac surgery, perfusionists play a pivotal role in managing the heart-lung machine, which temporarily takes over the patient’s circulatory and respiratory functions. ABG analysis provides the data needed to adjust pump flow rates, oxygen levels, and acid-base balance during CPB. Misinterpreting ABG results can lead to complications such as hypoxia, hypercapnia, or metabolic acidosis, all of which can jeopardize patient recovery.
This section explores why ABG interpretation for perfusionists is a cornerstone of successful cardiac procedures. From monitoring oxygenation during aortic valve replacement to managing pH levels during coronary artery bypass grafting (CABG), accurate interpretation ensures the perfusionist can respond swiftly to physiological changes. Let’s break down the key components of an ABG report and how they apply to your role.
What is an ABG Report?
An ABG report is a diagnostic test that measures the partial pressures of oxygen (PaO₂) and carbon dioxide (PaCO₂) in arterial blood, along with pH, bicarbonate (HCO₃⁻), and oxygen saturation (sO₂). Additional parameters, such as electrolytes (e.g., K⁺, Na⁺) and metabolites (e.g., lactate), provide a holistic view of the patient’s status. For perfusionists, these values guide intraoperative decisions, especially during CPB when the patient’s natural respiratory and circulatory systems are bypassed.
Role of Perfusionists in ABG Analysis
Perfusionists rely on ABG data to maintain homeostasis during cardiac surgery. This includes adjusting the oxygenator, managing carbon dioxide levels, and correcting acid-base imbalances. The ability to interpret ABG results accurately allows perfusionists to collaborate effectively with anesthesiologists and surgeons, ensuring the patient’s physiological needs are met throughout the procedure.
Key Components of ABG Interpretation for Perfusionists
To interpret ABG results effectively, perfusionists must understand each parameter and its implications during cardiac surgery. Let’s examine the core elements of an ABG report, using a sample case to illustrate practical application.
Sample ABG Report Analysis
Consider the following ABG results, typical of a cardiac surgery patient on CPB:
- pH: 7.361 (normal: 7.35–7.45)
- PaCO₂: 32.2 mmHg (normal: 35–45 mmHg)
- PaO₂: 317 mmHg (normal: 75–100 mmHg on room air)
- Oximetry: ctHb 8.1 g/dL, sO₂ 99.0%, FMetHb 2.1%
- Electrolytes: K⁺ 5.2 mmol/L, Na⁺ 128 mmol/L
- Metabolites: cGlu 200 mg/dL, cLac 2.2 mmol/L
- Acid-Base: cHCO₃⁻ 18.7 mmol/L, cBase -2.7 mmol/L
This sample report will serve as the foundation for our detailed interpretation, tailored to perfusionist needs.
pH and Acid-Base Status
The pH value (7.361) indicates the blood’s acidity or alkalinity. A normal range of 7.35–7.45 suggests no acute disturbance, but the low bicarbonate (18.7 mmol/L) and negative base excess (-2.7 mmol/L) point to compensated metabolic acidosis. For perfusionists, this could indicate inadequate tissue perfusion or lactic acid buildup during CPB. Monitoring and correcting pH is critical to prevent arrhythmias or organ dysfunction.
Oxygenation Parameters (PaO₂ and sO₂)
PaO₂ at 317 mmHg reflects high oxygen levels, likely due to supplemental oxygen during surgery. However, the elevated methemoglobin (FMetHb 2.1%) reduces oxygen-carrying capacity, a concern for perfusionists managing CPB. The sO₂ of 99.0% is reassuring, but the low hemoglobin (ctHb 8.1 g/dL) suggests anemia, necessitating adjustments in oxygen delivery.
Carbon Dioxide Levels (PaCO₂)
A PaCO₂ of 32.2 mmHg indicates mild hyperventilation, likely a compensatory response to metabolic acidosis. Perfusionists must adjust the ventilator settings or CO₂ sweep rate in the oxygenator to maintain optimal PaCO₂ levels, avoiding respiratory alkalosis or acidosis.
Electrolytes and Their Impact
Electrolyte imbalances, such as hyperkalemia (K⁺ 5.2 mmol/L) and hyponatremia (Na⁺ 128 mmol/L), can affect cardiac stability. Hyperkalemia, possibly from hemolysis or cardioplegia solutions, requires close monitoring to prevent arrhythmias during CPB.
Metabolites: Glucose and Lactate
Elevated glucose (200 mg/dL) and lactate (2.2 mmol/L) suggest stress-induced hyperglycemia and mild tissue hypoperfusion. Perfusionists should optimize pump flow and oxygen delivery to reduce lactate levels, collaborating with the surgical team to address underlying causes.
Step-by-Step ABG Interpretation Process for Perfusionists
Interpreting ABG results requires a systematic approach. Here’s a step-by-step guide tailored for perfusionists in the cardiac surgery setting:
Step 1: Assess pH for Acid-Base Status
Start with the pH to determine if the patient is acidotic (<7.35), alkalotic (>7.45), or normal (7.35–7.45). In our sample, a pH of 7.361 is normal, but the low HCO₃⁻ suggests a metabolic issue.
Step 2: Evaluate PaCO₂ for Respiratory Contribution
Check PaCO₂ to identify respiratory acidosis (>45 mmHg) or alkalosis (<35 mmHg). A value of 32.2 mmHg indicates respiratory compensation for metabolic acidosis.
Step 3: Analyze HCO₃⁻ and Base Excess for Metabolic Status
Low HCO₃⁻ (18.7 mmol/L) and a negative base excess (-2.7 mmol/L) confirm metabolic acidosis. This guides perfusionists to investigate perfusion adequacy during CPB.
Step 4: Review Oxygenation (PaO₂ and sO₂)
High PaO₂ (317 mmHg) and sO₂ (99.0%) are expected with supplemental oxygen, but elevated FMetHb (2.1%) and low ctHb (8.1 g/dL) require attention to optimize oxygen delivery.
Step 5: Consider Electrolytes and Metabolites
Address hyperkalemia, hyponatremia, hyperglycemia, and elevated lactate to prevent complications like arrhythmias or organ damage.
Clinical Implications of ABG Interpretation for Perfusionists
ABG interpretation directly influences perfusion strategies during cardiac surgery. Let’s explore how these findings impact patient management.
Managing Metabolic Acidosis During CPB
Compensated metabolic acidosis, as seen in the sample, may result from hypoperfusion or hemolysis. Perfusionists can increase pump flow, adjust the oxygenator, or administer bicarbonate under anesthesiologist guidance to correct the imbalance.
Addressing Anemia and Methemoglobinemia
The low hemoglobin (8.1 g/dL) and elevated methemoglobin (2.1%) suggest a need for transfusion consideration or investigation into causative agents (e.g., nitrates). Perfusionists must ensure adequate oxygen delivery despite these challenges.
Optimizing Ventilation and Oxygenation
High PaO₂ (317 mmHg) indicates effective oxygenation, but perfusionists should avoid hyperoxia, which can cause oxidative stress. Adjust FiO₂ and monitor sO₂ trends.
Electrolyte Management in the OR
Hyperkalemia (K⁺ 5.2 mmol/L) requires vigilant ECG monitoring and potential correction with insulin or calcium. Hyponatremia (Na⁺ 128 mmol/L) may need fluid management adjustments.
Advanced ABG Interpretation Techniques for Perfusionists
Beyond basic analysis, perfusionists can use advanced techniques to enhance decision-making during complex cardiac procedures.
Temperature-Corrected ABG Values
Temperature-corrected values (e.g., pH(T) 7.351) account for hypothermia during CPB. Perfusionists must interpret these alongside uncorrected values to guide therapy accurately.
Lactate Trends and Tissue Perfusion
Rising lactate levels (2.2 mmol/L in the sample) indicate poor tissue perfusion. Serial ABG measurements help perfusionists adjust pump flow and oxygen delivery to improve outcomes.
Integration with Hemodynamic Monitoring
Combine ABG data with hemodynamic parameters (e.g., mean arterial pressure, cardiac index) to assess overall perfusion status, a critical skill for perfusionists during CPB.
Common Pitfalls in ABG Interpretation for Perfusionists
Even experienced perfusionists can encounter challenges. Here are common pitfalls and how to avoid them:
Misinterpreting Compensatory Mechanisms
A low PaCO₂ (32.2 mmHg) might be mistaken for primary respiratory alkalosis. Always correlate with HCO₃⁻ and base excess to identify compensation for metabolic acidosis.
Overlooking Methemoglobinemia
Elevated FMetHb (2.1%) can be missed if not routinely checked. Regular oximetry analysis is essential to detect this condition early.
Ignoring Anemia’s Impact
Low ctHb (8.1 g/dL) can reduce oxygen delivery, yet it may be overlooked if PaO₂ and sO₂ appear normal. Integrate hemoglobin data into perfusion strategies.
Best Practices for ABG Interpretation in Cardiac Surgery
To excel in ABG interpretation for perfusionists, adopt these best practices:
Regular Training and Simulation
Participate in simulation-based training to practice ABG interpretation under realistic cardiac surgery scenarios.
Collaboration with the Surgical Team
Work closely with anesthesiologists and surgeons to correlate ABG findings with clinical observations and adjust CPB settings accordingly.
Use of Technology and Alerts
Leverage ABG analyzers with automated alerts for critical values (e.g., pH <7.2, K⁺ >5.5) to enhance real-time decision-making.
Case Studies: ABG Interpretation in Action
Case Study 1: CABG with Metabolic Acidosis
A 65-year-old patient undergoing CABG shows pH 7.30, PaCO₂ 28 mmHg, HCO₃⁻ 16 mmol/L, and lactate 3.5 mmol/L. The perfusionist increases pump flow and administers bicarbonate, resolving the acidosis within 30 minutes.
Case Study 2: Aortic Valve Replacement with Methemoglobinemia
During aortic valve replacement, a patient’s FMetHb rises to 3.0%. The perfusionist identifies a causative drug, adjusts therapy, and stabilizes oxygen delivery.
Future Trends in ABG Interpretation for Perfusionists
Advancements in ABG technology, such as continuous monitoring systems and AI-assisted interpretation, promise to enhance precision in cardiac surgery. Perfusionists should stay updated on these innovations to maintain cutting-edge skills.
Frequently Asked Questions About ABG Interpretation for Perfusionists
1. What is the formula for sweep and FiO₂ adjustment during CPB?
Answer:
Sweep gas flow and FiO₂ (fraction of inspired oxygen) adjustments are critical for managing PaCO₂ and PaO₂ during CPB.
- Sweep Gas Flow (to control PaCO₂): Sweep flow (in liters per minute, L/min) is typically set at a 1:1 ratio with blood flow (e.g., if blood flow is 4 L/min, start with a sweep of 4 L/min). To adjust PaCO₂:
- Increase sweep flow to decrease PaCO₂ (e.g., by 10–20% if PaCO₂ is >45 mmHg).
- Decrease sweep flow to increase PaCO₂ (e.g., by 10–20% if PaCO₂ is <35 mmHg).
- FiO₂ Adjustment (to control PaO₂): FiO₂ is adjusted to maintain PaO₂ between 150–250 mmHg during CPB.
- If PaO₂ <150 mmHg, increase FiO₂ by 0.1–0.2 (e.g., from 0.6 to 0.8).
- If PaO₂ >250 mmHg, decrease FiO₂ by 0.1–0.2 to avoid hyperoxia.
Always monitor ABG results every 15–30 minutes to fine-tune settings.
2. What are the formulas for potassium and bicarbonate addition during CPB?
Answer:
Electrolyte and acid-base corrections are vital during CPB.
- Potassium (K⁺) Addition: To correct hyperkalemia or hypokalemia:
- Formula: K⁺ dose (mEq) = [Desired K⁺ – Actual K⁺] × Weight (kg) × 0.3 (where 0.3 is the distribution volume of K⁺).
- Example: If K⁺ is 5.2 mmol/L, desired K⁺ is 4.0 mmol/L, and patient weight is 70 kg:
Dose = (4.0 – 5.2) × 70 × 0.3 = -25.2 mEq (indicating a need to lower K⁺, e.g., with insulin/dextrose). - Add potassium chloride (KCl) slowly via the CPB circuit if K⁺ is low.
- Bicarbonate (HCO₃⁻) Addition: To correct metabolic acidosis:
- Formula: HCO₃⁻ dose (mEq) = Base Deficit × Weight (kg) × 0.3 (where 0.3 is the extracellular fluid volume).
- Example: If base deficit is -2.7 mmol/L and patient weight is 70 kg:
Dose = 2.7 × 70 × 0.3 = 56.7 mEq of sodium bicarbonate. Administer half the dose over 10–15 minutes, recheck ABG, and adjust.
Always coordinate with the anesthesiologist before administering.
3. Why is ABG interpretation important for perfusionists during cardiac surgery?
Answer:
ABG interpretation allows perfusionists to monitor oxygenation (PaO₂, sO₂), ventilation (PaCO₂), and acid-base status (pH, HCO₃⁻) during CPB. It helps adjust pump settings, oxygenator performance, and fluid management to prevent complications like hypoxia, acidosis, or arrhythmias, ensuring patient stability throughout the procedure.
4. How do perfusionists identify compensated metabolic acidosis on an ABG report?
Answer:
Compensated metabolic acidosis is identified when pH is normal (7.35–7.45), but HCO₃⁻ is low (<22 mmol/L) and PaCO₂ is low (<35 mmHg). For example, a pH of 7.361, HCO₃⁻ of 18.7 mmol/L, and PaCO₂ of 32.2 mmHg indicate metabolic acidosis with respiratory compensation (hyperventilation to lower PaCO₂).
5. What should perfusionists do if methemoglobin (FMetHb) levels are elevated?
Answer:
Elevated FMetHb (e.g., 2.1%, normal <1%) reduces oxygen-carrying capacity. Perfusionists should:
- Identify potential causes (e.g., drugs like nitrates or local anesthetics).
- Notify the anesthesiologist to consider methylene blue (1–2 mg/kg IV) if levels exceed 5%.
- Optimize oxygen delivery via the CPB circuit by increasing FiO₂ or pump flow.
6. How does anemia affect ABG interpretation for perfusionists?
Answer:
Low hemoglobin (e.g., ctHb 8.1 g/dL) reduces oxygen-carrying capacity, even if PaO₂ and sO₂ are normal. Perfusionists should monitor oxygen content (ctO₂c) and consider transfusion if hemoglobin falls below 7–8 g/dL, ensuring adequate tissue perfusion during CPB.
7. What are the risks of hyperkalemia during cardiac surgery, and how can perfusionists manage it?
Answer:
Hyperkalemia (e.g., K⁺ 5.2 mmol/L) can cause arrhythmias, especially during CPB. Perfusionists should:
- Monitor ECG for peaked T-waves or widening QRS.
- Use insulin/dextrose or calcium gluconate to stabilize cardiac membranes.
- Avoid excessive potassium in cardioplegia solutions and recheck ABG frequently.
8. How can perfusionists use lactate levels in ABG to assess tissue perfusion?
Answer:
Elevated lactate (e.g., 2.2 mmol/L, normal 0.5–2.0 mmol/L) indicates tissue hypoperfusion or anaerobic metabolism. Perfusionists can increase pump flow, optimize oxygen delivery, and address underlying causes (e.g., low cardiac output). Serial lactate measurements help track perfusion trends during surgery.
9. What is the significance of temperature-corrected ABG values during CPB?
Answer:
Temperature-corrected ABG values (e.g., pH(T) 7.351) adjust for hypothermia during CPB, which affects pH and gas solubility. Perfusionists should compare corrected and uncorrected values to guide acid-base management, ensuring decisions align with the patient’s actual physiological state.
10. How often should perfusionists perform ABG analysis during cardiac surgery?
Answer:
Perfusionists should perform ABG analysis every 15–30 minutes during CPB, or more frequently if there are significant changes in pH, PaCO₂, PaO₂, or clinical status. Regular monitoring ensures timely adjustments to sweep flow, FiO₂, and acid-base corrections.
Conclusion: Mastering ABG Interpretation for Perfusionists
ABG interpretation for perfusionists is a vital skill that ensures patient safety and optimal outcomes in cardiac surgery. By understanding pH, oxygenation, CO₂ levels, electrolytes, and metabolites, perfusionists can fine-tune CPB management and collaborate effectively with the surgical team. Use the insights from this guide to enhance your practice on cardiperf.com, and continue learning to stay ahead in this dynamic field.
For more resources and updates, explore our website and join our community of cardiac surgery professionals dedicated to excellence.