Postoperative hemorrhage is one of the most critical challenges in cardiac surgery, impacting patient outcomes, ICU resources, and overall healthcare costs. This blog dives into the causes, case studies, and strategies to manage this complication effectively. Designed for perfusionists, surgeons, anesthesiologists, and other cardiac care professionals, this guide offers actionable insights to improve care quality.
Understanding Postoperative Hemorrhage in Cardiac Surgery
What is Postoperative Hemorrhage?
Postoperative hemorrhage refers to excessive bleeding following a surgical procedure. In cardiac surgery, it can arise due to incomplete hemostasis, coagulopathies induced by cardiopulmonary bypass (CPB), or patient-specific factors like advanced age and comorbidities.
Why Does it Matter?
- Increased morbidity and mortality risk.
- Prolonged ICU stays and higher healthcare costs.
- Greater reliance on transfusion, which carries its risks.
Primary Causes of Hemorrhage in Cardiac Surgery
- Surgical Factors
- Technical errors such as incomplete hemostasis or graft site bleeding.
- Adhesions or injuries to adjacent tissues during retraction.
- Coagulation Disorders
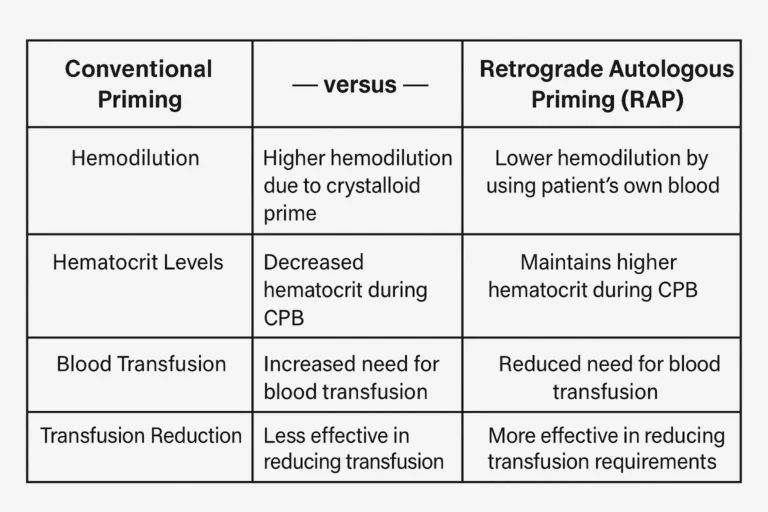
- Dilutional coagulopathy from excessive crystalloid infusion.
- Platelet dysfunction due to CPB and exposure to non-physiological surfaces.
- Medication-Related Factors
- Antiplatelet agents (e.g., aspirin, clopidogrel) increasing bleeding risks.
- Inadequate reversal of anticoagulants like heparin post-procedure.
- Delayed Recognition
- Minimal chest tube output masking ongoing internal bleeding.
- Lack of thorough inspection during the surgical close.
Case Study: Learning from a Complex Scenario
A 75-year-old male undergoing coronary artery bypass grafting (CABG) developed a postoperative complication despite an uneventful surgery. The ICU team noticed clinical signs of hypovolemia and hypotension with minimal chest tube drainage. A bedside X-ray revealed right-sided fluid collection due to unnoticed bleeding into the pleural space.
Management Steps:
- Immediate chest tube placement to relieve pleural effusion.
- Re-exploration identified and resolved the bleeding source.
- Comprehensive post-repair hemostasis ensured no further issues.
Best Practices for Managing Postoperative Hemorrhage
- Intraoperative Precision
- Conduct thorough hemostasis checks before closure.
- Use adjuncts like fibrin sealants or topical hemostatic agents.
- Pay special attention to graft sites and the internal thoracic artery bed.
- Early Recognition and Monitoring
- Use continuous monitoring for hemodynamic instability.
- Implement point-of-care testing like thromboelastography (TEG) to assess coagulation.
- Encourage ICU staff to report even subtle changes in drainage or patient status.
- Multidisciplinary Collaboration
- Ensure seamless communication among surgeons, perfusionists, anesthesiologists, and ICU nurses.
- Use structured debrief protocols to streamline hemorrhage management.
- Rapid Re-Exploration Protocols
- Establish low thresholds for surgical re-exploration when bleeding persists.
- Evidence shows early intervention reduces complications and mortality rates.
- Optimized Postoperative Protocols
- Integrate hemostasis checklists into standard care protocols.
- Train staff to recognize and escalate care for suspected hemorrhage promptly.
Prevention Strategies
- Preoperative Assessment
- Assess bleeding risks by reviewing the patient’s medication history and coagulation profile.
- Stop antiplatelet drugs per guidelines, balancing bleeding and thrombotic risks.
- Anticoagulation Management
- Use tailored heparin protocols during CPB and ensure proper reversal post-bypass.
- Monitor ACT and ABGs for early signs of bleeding tendencies.
- Post-Operative Care
- Set clear monitoring protocols, emphasizing vigilance in the first 24 hours.
- Use imaging (X-ray, ultrasound) routinely to identify hidden complications.
The Role of Perfusionists in Managing Hemorrhage
Perfusionists are crucial in mitigating hemorrhagic risks during and after CPB. By ensuring optimized perfusion parameters and closely monitoring coagulation profiles, perfusionists can significantly impact patient outcomes. Key responsibilities include:

- Managing anticoagulation and ACT levels during bypass.
- Balancing fluid replacement to avoid dilutional coagulopathy.
- Collaborating with the surgical team to adjust strategies in real-time.
FAQs on Postoperative Hemorrhage Management
Q1: What is the role of TEG in cardiac surgery?
A: TEG provides real-time insights into coagulation status, helping guide transfusion and pro-hemostatic therapy decisions.
Q2: When should re-exploration be considered?
A: Persistent bleeding (>200 mL/hour), hemodynamic instability, or signs of tamponade warrant immediate surgical review.
Q3: How can hidden bleeding sites be identified?
A: Use bedside imaging (e.g., ultrasound, chest X-ray) and closely monitor clinical signs like tachycardia or hypotension.
Conclusion
Managing postoperative hemorrhage in cardiac surgery demands a proactive, multidisciplinary approach. By focusing on prevention, early detection, and effective response strategies, healthcare teams can improve patient outcomes and reduce complications.
At CardiPerf.com, we are committed to empowering cardiac surgery professionals with the latest insights, tools, and techniques. Stay tuned for more resources to enhance your expertise and elevate patient care.