Introduction
Systemic air embolism is a potentially devastating complication during cardiac surgery, often resulting in severe morbidity or mortality if not promptly addressed. The multidisciplinary surgical team—including cardiac surgeons, anesthesiologists, perfusionists, and operating room nurses—plays a critical role in preventing, detecting, and managing this emergency. However, errors or lapses in judgment by any team member can inadvertently contribute to this condition.
This article examines the causes, prevention strategies, and management of systemic air embolism, while shedding light on how malpractice or technical oversights by anesthesiologists and cardiac surgeons can contribute to its occurrence.
What Is Systemic Air Embolism?
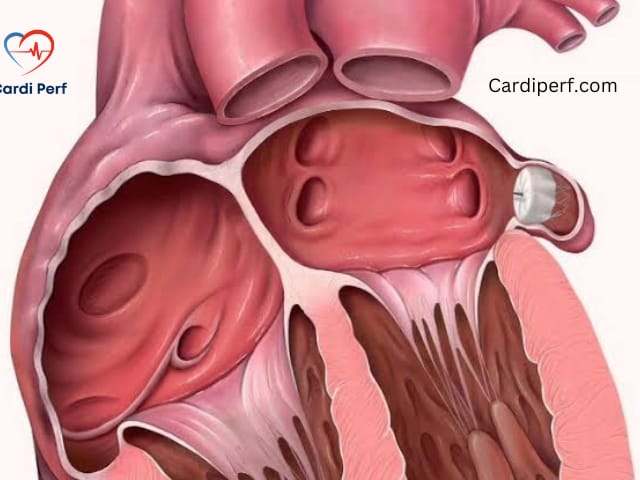
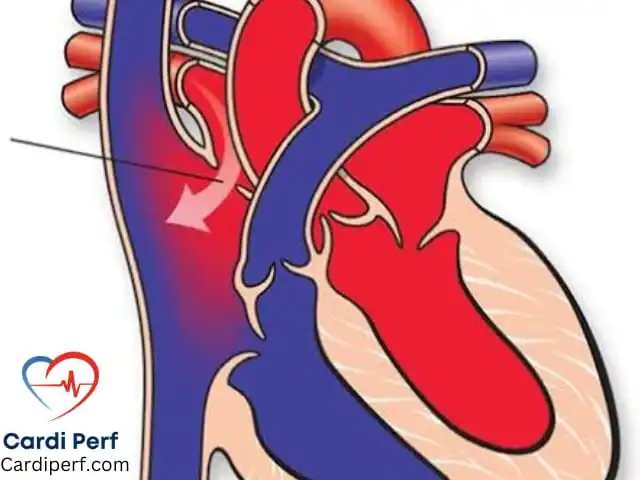
Systemic air embolism occurs when air enters the vascular system and travels to vital organs, such as the brain, heart, or kidneys, causing ischemia and organ dysfunction. The condition is particularly concerning in cardiac surgery due to the use of cardiopulmonary bypass (CPB), where air can inadvertently enter through various pathways.
All Possible Causes of Systemic Air Embolism
1. Air Entry into the CPB Circuit
- Improper priming of the CPB circuit, leading to residual air in venous or arterial lines.
- Pressurization of non-vented cardiotomy reservoirs or arterial filters, allowing air ingress.
- Failure of bubble detectors or lack of alarms to detect air in the CPB system.
2. Surgical Technique Errors
- Incomplete de-airing of cardiac chambers, bypass grafts, or the aorta before concluding surgery.
- Aspiration of air through coronary arteriotomies or during venting procedures.
- Inadvertent introduction of air during removal of aortic clamps or closure of graft sites.
3. Anesthesia-Related Errors
- Mismanagement of Transesophageal Echocardiography (TEE): Inadequate monitoring or failure to detect residual air in the heart chambers or great vessels.
- Air in Intravenous (IV) Lines: Accidental infusion of air into venous lines, particularly during transfusion or administration of fluids.
- Patient Positioning Errors: Improper positioning during surgery, such as failure to use the Trendelenburg position when air embolism is suspected, allowing air to migrate toward the brain.
4. Cardiac Surgeon-Related Errors
- Incomplete De-airing Protocols: Neglecting to perform rigorous de-airing steps, such as ballottement of the heart, inversion of the left atrial appendage, and needle venting of the left ventricle.
- Improper Closure of Grafts or Chambers: Residual air trapped in bypass grafts or cardiac chambers due to insufficient attention to detail during suturing or closure.
- Forgetting to Check Lines: Overlooking the direction of flow in perfusion or venting lines, which can lead to air inadvertently being infused into the heart.
5. Equipment Failures and Monitoring Gaps
- Malfunctioning bubble sensors or pump shut-off systems, resulting in undetected air entry.
- Emptying of the oxygenator without appropriate alarms, leading to air being pumped into the patient’s circulation.
- Disconnected or reversed lines in the CPB circuit.
6. Deep Hypothermia and Circulatory Arrest
- Air retention in the vascular system due to profound cooling and subsequent vasoconstriction.
7. Patient-Specific Factors
- Presence of a patent foramen ovale (PFO), allowing air to bypass the pulmonary circulation and directly enter the systemic circulation.
How Anesthesia Malpractice Can Contribute to Systemic Air Embolism
Anesthesiologists play a critical role in monitoring the patient’s hemodynamics, ensuring proper positioning, and using imaging tools like TEE to detect air. However, lapses or errors can have significant consequences:
1. TEE Mismanagement
- Failing to use TEE effectively to detect and quantify residual air during or after de-airing procedures can result in undetected air embolism.
- Misinterpretation of TEE findings may lead to premature closure of the chest, leaving air in the cardiac chambers or great vessels.
2. Infusion Errors
- Allowing air bubbles to enter IV lines during administration of medications, fluids, or transfusions.
- Neglecting to check for air in blood reservoirs or infusion systems, particularly when returning residual blood from the CPB oxygenator.
3. Improper Ventilation Strategies
- Inadequate management of ventilation settings during periods of air embolism risk, such as during weaning from CPB.
4. Positional Mistakes
- Failure to position the patient appropriately in Trendelenburg or left lateral decubitus positions when air embolism is suspected, allowing air to travel to critical areas such as the brain or heart.
How Cardiac Surgeon Malpractice Can Contribute to Systemic Air Embolism
Cardiac surgeons must adhere to strict protocols to prevent air embolism during surgery. Common errors include:
1. Incomplete De-airing
- Neglecting to invert the left atrial appendage or thoroughly vent the left ventricle.
- Failing to adequately inspect bypass grafts and the aortic root for trapped air.
2. Premature Decannulation
- Decannulating the patient and closing the chest without ensuring all air has been evacuated from the cardiac chambers, aorta, and grafts.
3. Mismanagement of Graft Placement
- Inadequate sealing of bypass grafts, allowing air to enter the coronary circulation.
- Errors in connecting or flushing grafts, leaving residual air that can travel to the heart or systemic circulation.
4. Failure to Verify CPB Circuit Integrity
- Overlooking potential leaks or loose connections in the CPB system.
- Improperly primed circuits that leave air bubbles undetected.
FAQs: Addressing Common Concerns
1. How can systemic air embolism be prevented in cardiac surgery?
Prevention requires meticulous adherence to de-airing protocols, vigilant CPB circuit monitoring, and effective use of TEE for real-time detection of air.
2. What are the signs of systemic air embolism during surgery?
Signs include sudden hypotension, arrhythmias, cyanosis, ventricular fibrillation, and neurological deficits like seizures or loss of consciousness.
3. What is the role of anesthesiologists in managing air embolism?
Anesthesiologists monitor for air using TEE, optimize patient positioning, and administer medications such as steroids, mannitol, or thiopental to minimize damage.
4. Can malpractice lead to systemic air embolism?
Yes, errors in de-airing, monitoring, or surgical techniques by anesthesiologists or cardiac surgeons can inadvertently cause or exacerbate systemic air embolism.
5. How is systemic air embolism treated during surgery?
Treatment includes immediate cessation of arterial perfusion, Trendelenburg positioning, reinstitution of CPB, evacuation of air, and administration of neuroprotective agents.
Conclusion
Systemic air embolism is a catastrophic but preventable complication of cardiac surgery. By recognizing the potential contributions of anesthesiologists and cardiac surgeons to its occurrence, the surgical team can take steps to minimize risks through meticulous preparation, vigilant monitoring, and adherence to established protocols. Preventing systemic air embolism requires a collaborative approach, where every member of the team plays their part in ensuring patient safety and optimal surgical outcomes.
For more insights on cardiac surgery emergencies, visit cardiperf.com.