Introduction
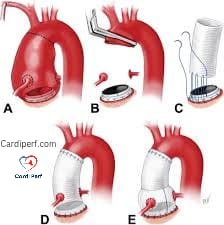
Redo cardiac surgeries, particularly those involving aortic root procedures, present unique challenges in myocardial protection. Patients with prior homograft aortic valve replacements often develop calcified roots and severe regurgitation, complicating surgical strategies. Additionally, previous coronary artery bypass grafts (CABG) can alter myocardial perfusion, requiring meticulous cardioplegia delivery to ensure adequate myocardial preservation.
Case Presentation
A 68-year-old male presents with a degenerated homograft aortic valve replacement performed 15 years prior. The valve has severe regurgitation, and the homograft root is extensively calcified. The patient also has a left internal thoracic artery (LITA) graft to the left anterior descending (LAD) artery, which is totally occluded proximally but well perfused by the graft. Antegrade cardioplegia is ineffective due to significant aortic insufficiency, and initial retrograde catheter placement attempts are unsuccessful.
Myocardial Protection Strategy
Given the failure of retrograde coronary sinus catheter placement through the right atrium, an alternative approach is necessary. The optimal strategy involves:
1. Direct Coronary Sinus Cannulation
- Conversion from a two-stage venous cannula to superior vena cava (SVC) and inferior vena cava (IVC) cannulation.
- Institution of cardiopulmonary bypass (CPB) with caval snares to prevent air embolism.
- Aortic cross-clamping and opening the right atrium under controlled conditions.
- Direct visualization and secure placement of the retrograde cardioplegia catheter in the coronary sinus with a purse-string suture to ensure effective delivery.
2. Avoidance of Myocardial Stunning
- Ensuring adequate myocardial cooling to reduce metabolic demand.
- Monitoring of transesophageal echocardiography (TEE) to confirm catheter placement and optimize perfusion.
- Adjusting retrograde cardioplegia pressure to prevent coronary sinus injury.
3. Alternative Strategies
- Maintaining ITA Perfusion: Systemic cooling (32-34°C) while allowing LITA perfusion to the LAD territory with concurrent retrograde cardioplegia for the remaining myocardium.
- Hybrid Cardioplegia Delivery: Combining direct ostial cardioplegia for the right coronary artery and retrograde cardioplegia for the left ventricle, ensuring full myocardial protection.
Femoral Cannulation and Difficult Sternotomy
Redo sternotomies are often challenging due to extensive adhesions and the risk of injuring underlying cardiac structures. In such cases, femoral cannulation serves as an essential alternative for initiating cardiopulmonary bypass before sternotomy.
- Benefits of Femoral Cannulation:
- Allows for controlled perfusion before sternotomy, minimizing hemodynamic instability.
- Reduces the risk of right ventricular or aortic injury during re-entry.
- Facilitates quick establishment of cardiopulmonary bypass in emergencies.
- Challenges:
- Increased risk of limb ischemia, requiring distal perfusion strategies.
- Possibility of retrograde aortic dissection in patients with severe atherosclerosis.
- Limited accessibility in obese or peripheral vascular disease patients. In complex redo procedures, femoral cannulation remains a valuable option when standard central cannulation is deemed high-risk.
Discussion
Effective myocardial protection is paramount in complex redo surgeries, particularly in patients with severe aortic regurgitation and prior CABG. Antegrade cardioplegia is unreliable in these cases, necessitating retrograde perfusion. Failure of catheter placement due to anatomical variations, such as a small coronary sinus or a Chiari network, requires direct exposure for secure placement.
TEE guidance significantly improves retrograde catheter insertion success and ensures optimal myocardial perfusion. If the coronary sinus diameter is <8mm, smaller manually inflated balloon catheters can be used. Direct right atrial exposure provides the best option for securing catheter placement and optimizing cardioplegia delivery.
In cases where ITA grafts provide sole perfusion to critical myocardial regions, controlled systemic cooling with unimpeded ITA flow can be considered. However, complete electromechanical arrest is often preferred in complex surgeries, making controlled ITA occlusion with a bulldog clamp the better option.
Conclusion
Redo aortic root surgery with prior CABG requires a tailored approach to myocardial protection. Retrograde cardioplegia remains the cornerstone strategy, with direct coronary sinus cannulation being necessary in difficult cases. Utilizing TEE, systemic cooling, and hybrid cardioplegia techniques can further enhance myocardial protection, ensuring optimal surgical outcomes.
FAQs on Myocardial Protection in Redo Cardiac Surgery
1. Why is myocardial protection critical in redo cardiac surgery?
Myocardial protection ensures adequate oxygen delivery and prevents ischemia-related damage during cross-clamping and cardiopulmonary bypass.
2. Why is antegrade cardioplegia ineffective in cases of severe aortic insufficiency?
The regurgitant valve prevents the cardioplegia solution from adequately perfusing the myocardium, leading to suboptimal protection.
3. What are the challenges of retrograde cardioplegia delivery?
Difficulties in cannulation due to anatomical variations, small coronary sinus orifice, or the presence of a Chiari network can impede effective delivery.
4. How does transesophageal echocardiography (TEE) assist in retrograde cannulation?
TEE helps guide catheter placement, confirms positioning, and ensures adequate retrograde cardioplegia delivery.
5. What are the risks of prolonged ischemic time?
Prolonged ischemia can lead to myocardial stunning, necrosis, and increased risk of postoperative heart failure.
6. Why is systemic cooling used during myocardial protection?
Cooling reduces myocardial metabolic demand, extending safe ischemic time and improving myocardial preservation.
7. How is the LITA managed in redo cardiac surgery?
It can be either controlled with a bulldog clamp to achieve full arrest or left open to perfuse the LAD while the rest of the heart is protected via retrograde cardioplegia.
8. What are alternative cardioplegia delivery methods?
Direct ostial infusion, hybrid cardioplegia (antegrade and retrograde combination), and controlled systemic perfusion are viable alternatives.
9. What complications can arise from retrograde cardioplegia?
Coronary sinus injury, inadequate perfusion to certain myocardial territories, and catheter malposition are potential risks.
10. What is the optimal temperature for systemic cooling?
The commonly used range is 32-34°C, but deeper hypothermia may be used in prolonged procedures based on surgeon preference.
About Us
At CardiPerf.com, we are dedicated to providing cutting-edge insights into perfusion sciences, cardiac surgery, and extracorporeal technologies. Our goal is to bridge the gap between clinical expertise and the latest advancements in myocardial protection, ensuring that perfusionists, surgeons, and healthcare professionals stay informed with evidence-based practices. Whether you are looking for research-backed articles, in-depth surgical guides, or expert opinions, CardiPerf.com serves as your premier resource for everything related to cardiovascular perfusion.